
Related Content
-
Social Network Strategy: Turning the Tables on HIV
-
By Joan Singson | February 25, 2015
Program Manager, ETRI used to walk in and out of drab motels and dive bars in the middle of the night, distributing condoms and encouraging people to test for HIV. Yup! Been there, done that. The strategies we used to help reduce the spread of HIV in the early 1990’s were not for the faint of heart.
Those of us who were involved back when old school was hip hop and Wu-Tang-Clan was the bomb could probably rattle off a hundred ways to recruit individuals for HIV counseling, testing and referral. Organizations were motivated by the message that “anyone can get HIV,” and funding streams asked them to cast a wide net and bring in as many individuals as possible for testing.
Since then, the business of recruitment has evolved.
- Read More
Related Content
HIV Treatment: Keeping People in Care

By BA Laris, MPH | March 12, 2015
Research Associate, ETR
In recent years, there has been a major shift in the way we approach HIV treatment and prevention. Research has shown (for example, see Gardner’s 2011 report here; and the AIDS.gov background here) that we will have our greatest impact when we focus on two major steps.
- Locate individuals at greatest risk for HIV and motivate them to get tested.
- Connect with individuals who have HIV and provide support for them to start and stay in HIV-related medical treatment.
These are deceptively simple prescriptions. But if you work in HIV care and treatment settings, you know there are a myriad of physical, social and emotional issues that can make it difficult for people to stay engaged in continuous treatment. This challenge is one that our Community Impact Solutions team addresses in our work providing capacity building for community-based organizations. We develop strategies and deliver coaching and support to strengthen HIV programs. Our approaches are both research proven and real-world practical.
The Challenge
Today’s HIV medications make it possible for people living with HIV to dramatically decrease the amount of virus in their blood. This can make the disease almost undetectable. Treatment helps people live longer, healthier lives and strongly reduces the likelihood that they will pass the virus on to others.
But there’s a catch. People have to stay in regular medical care, taking medications consistently, for the rest of their lives.
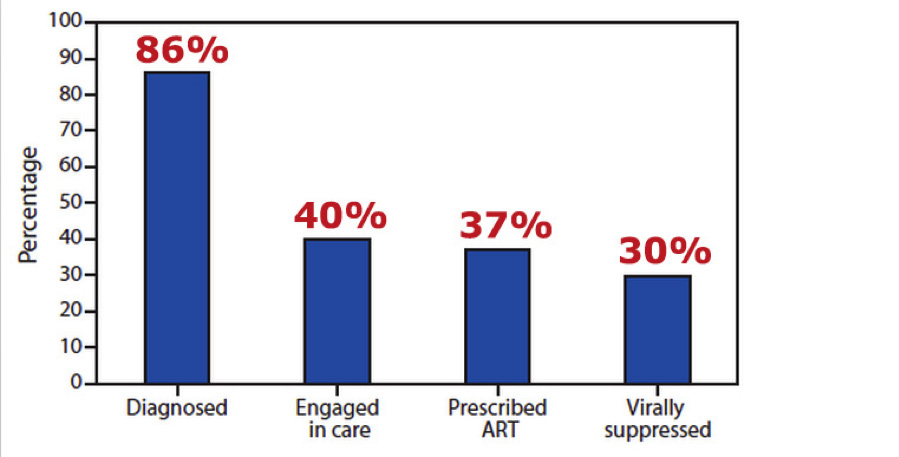
For some people, this is manageable. About 30% of people with HIV in the United States are currently at the stage of viral suppression—they’ve tested positive, they’ve been evaluated medically, they’re taking their medications daily and their viral load is very low.
But for others, the idea of showing up at the doctor’s office regularly and taking medicines every day is absolutely unimaginable!
The HIV Care Continuum
Today, most people living with HIV in the U.S. are not receiving adequate treatment.
- About 1 in 7 isn’t aware of his or her HIV status.
- Among those who have tested HIV-positive, fewer than half have started medical care for the disease.
- Many of those who initially seek care either don’t start medicines, or don’t continue them. They may skip appointments or stop seeing their medical provider altogether.
This range of health outcomes is often called the HIV Care Continuum or the HIV Treatment Cascade. Here’s what it looks like:
Estimated percentage of persons living with HIV, by outcome along the HIV Care Continuum
United States, 2011
Let’s Figure It Out!
I actually get really excited about the challenges illustrated in the Continuum of Care. I like figuring out ways to translate research and science into practical, easily accessible tools for real-world settings. Recently, I’ve been providing capacity-building assistance to community-based organizations addressing this issue of retention in HIV care.
I’ve worked with our team to develop tools and resources for peer navigators, linkage coordinators and clinicians. One of the first things we’ve learned to examine is who is most likely to “fall out of care.”
The research (and practical experience) shows this tends to be people:
- of color
- in poverty
- who are homeless
- with mental illness
- with substance abuse problems
- who are young
- who are transgender
Those who have higher CD4 counts when they are diagnosed are also more likely to fall out of care. The CD4 count is a measure of the immune system’s health. When those numbers are high, people with HIV usually feel healthy. It’s often difficult for them to make the effort to engage in treatment and follow through on the commitment to take medicines every day when they don’t really believe they’re sick.
Making the Cascade Local
One of the interesting things we’ve been asking providers to do is make this cascade concept local. When they look at their own program utilization data, who is most likely to drop out of care?
We then ask them to use our Retention Risk Indicator Tool to identify and develop specific strategies to intervene and address barriers when people are first engaged in care. The tool helps providers examine three typical categories of barriers to care:
- Structural. This includes such things as organizational problems, unavailable services, inconvenient location, long wait times, inconvenient appointment times and language barriers.
- Financial. This includes items such as lack of insurance, underinsurance or the cost of services. It might also include costs related to childcare, transportation or missing time at work.
- Personal/Cultural. This addresses a client’s knowledge, attitudes and beliefs about HIV and health care, as well as cultural barriers and experiences with racism, sexism, homophobia and/or transphobia.
Making Connections
If there is just one thing we need to remember in this light—something both research and our own common sense tells us—it’s that connection makes a difference. A person’s connection to his or her provider is vital to retention in care.
When people trust their provider—this includes believing their provider cares genuinely for them and has their best interest as a priority—they are more likely to follow treatment guidelines and keep coming back.
Impressive Examples
We’ve worked with a number of organizations who are doing amazing work with their clients. We’ve seen some highly creative strategies for increasing connection with clients and enhancing retention in care. For example:
- An organization in Florida has peer navigators make home visits after the first medical appointment. This is an effective way to build stronger connections, especially with clients who are recently arrived immigrants. This strategy resulted in increased returns for follow-up care.
- A community-based organization in rural Wisconsin developed a close partnership with a mobile substance use treatment clinic. They offer priority access to clients of the mobile clinic. It is much easier for these clients to begin and continue HIV treatment.
- A New York clinic developed a series of fun, informative videos for their waiting room. This creates a welcoming and engaging atmosphere and helps clients feel more comfortable talking to their medical provider.
Solutions: Realistic and Local
There is no one-size-fits-all solution for increasing retention. The realities of each community are distinct and uniquely influence the barriers people face.
Local solutions need to be developed to address local challenges. These should be informed by research, reports from the field (e.g., other successful projects), and the experience and expertise of local providers and community leaders. The examples above show that creativity and ingenuity have an important role to play. These efforts make a real difference in clients’ lives.
It’s also important to monitor and evaluate both new and ongoing strategies to ensure that scarce resources are being used most effectively.
Our capacity-building team at ETR provides free assistance to HIV prevention organizations funded by the Centers for Disease Control and Prevention, Division of HIV/AIDS Prevention. We love sharing these dynamic and effective strategies for HIV prevention.
BA recently did a video for us describing Retention in Care and her trainings addressing this strategy. Check it out!
BA Laris, MPH, is a Research Associate at ETR. She provides capacity-building assistance to community-based organizations working in HIV prevention and has also worked in program planning, management and evaluation in the areas of HIV/AIDS, substance use prevention and treatment, and international health. She can be reached at bal@etr.org.



