
Related Content
Tic-Tic Boom: Being the Work and Doing the Work

By Michael Everett, MHS | October 29, 2015
Project Coordinator, ETR
What responsibility do HIV/AIDS organizations have concerning the wellness of staff who are also Black men who have sex with men?
I have pondered this question often throughout my 15-year career in HIV services. In that time, I have served as an outreach worker, health educator, case manager, assistant director and even a national capacity-builder.
Within each role, I have experienced something seen by many other BMSM struggling to make an impact on communities most burdened by HIV. This is the emergence of tokenism, isolation and control—or, as I like to refer to it, tic-tic boom.
Some of you might be familiar with tic-tic boom. It’s an expression that describes an instability that often leads to problematic outcomes. Have you ever had a friend who easily engages in conflicts and outbursts? Well, that might be an example of tic-tic boom.
And why would BMSM service providers have a tic-tic boom experience? Let’s take a look.
Tic: "T" Stands for Tokenism
Among BMSM service providers, some of us are hired because of our skill set. However, many of us are also partly or solely employed due to our access to a certain target population (that is, BMSM). In these circumstances, we can become tokenized—which represents the “T” in tic.
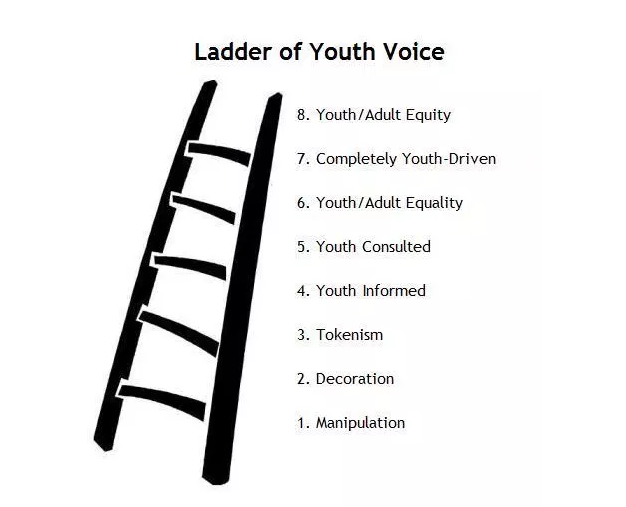
I have experienced this type of tokenism myself, although I had no language for it at the time. It wasn’t until I came across the Ladder of Participation in a professional development training that I understood what was happening. I was being invited to serve on LGBT community boards and sent to conferences to represent our youth program, but I was not educated on how to exist and contribute in a meaningful way.
 Then I realized that my participation at that level was never the intention. My job was to smile for pictures and be ready to serve as an example of how the agency was “transforming” my community.
Then I realized that my participation at that level was never the intention. My job was to smile for pictures and be ready to serve as an example of how the agency was “transforming” my community.
The Ladder of Participation was a critical tool in my understanding of this phenomenon. It helped reform my expectations—not just to be invited to a space, but to hold the powers that others held, be accountable through my own opinions and ideas, and be willing to share my concerns despite fear of recourse.
This process freed me from the idea others had, and that I’d perpetuated, that I was only to be seen and not truly heard.
Tic: “I” Stands for Isolation
Many people in this field are unaware of the isolation faced by BMSM service providers. It stems from having one’s personal social network deeply intertwined with one’s work. Boundaries are instituted both consciously and subconsciously in order to preserve one’s job.
For example, I was 18 years old when I first started doing HIV work. I worked for an organization designed to address HIV among “gay” youth. One of the immediate shifts I noticed was that my friends began to see me as an HIV expert. That was great. They were the target population, and I had access to them in a way that other staff members did not.
Learn about Community Impact Solutions Program's Intentional Leadership in Healthy Organizations webinar series here. You can view a recording of the first webinar, which expands on ideas in this blog post, here.
But this also meant that I was providing HIV testing and education to my peers in a professional capacity. I had access to information I wouldn’t have necessarily had otherwise—things such as HIV status, sexual activity and a general idea of whom my client/peers were engaging in sex with.
As I attempted to have a healthy social and dating life of my own, things became complicated due to my access to this information. I would often know when someone who was HIV-positive was sexually involved with a friend or family member who was not. I might know that the couple had unprotected sex. I might know that the HIV-positive person had not disclosed his status to my friend. But I was sworn to privacy.
Over time, this burden became more and more troubling. I slowly began to disengage from my community.
My isolation experience is not unusual among BMSM service providers. It can go on for years. We sometimes seek relief in unrealistic long-distance relationships (many times with other HIV service providers) that take us out of our local community. Some of us seek risky anonymous sexual encounters in an effort to set aside the personal information we’ve acquired about friends.
I have learned that isolation can facilitate and/or reinforce depression as well.
Tic: “C” Stands for Control
The “C” in tic is control. This refers to the growing awareness that, as tokens, we receive more scrutiny from peers and colleagues. Our capabilities are often questioned. That realization can promote defense mechanisms that cause us to break some personal and professional boundaries. It can lead to extreme people-pleasing—saying “yes” more often then we need to, or even should—in order to control perceptions others may have about our abilities.
I can recall a period in my life where I was coordinator for an agency in Philadelphia. My role was to conduct workshops around sexual and social health for young people in schools and community-based institutions. At a certain point I was conducting 7 to10 workshops a week.
In fact, I didn’t just conduct them. I created them, and I gave it my all like a good worker should. The requests never diminished because I loved what I did, I was good at it and there was always a need for more.
My superiors knew that our whole team of young people was burnt out, but saying “no” never seemed like an option. We were a nonprofit whose funding felt tentative, and we carried that weight on our shoulders. During one hectic week, I literally had a nervous breakdown in the middle of a session. I had to be escorted home. I rested for a day. Then I went back to work.
I’m not suggesting that my organization did not care. They most certainly did. But, like many AIDS service organizations, we were established out of crisis, so we continued to work every day as if we were in crisis. Unfortunately, that mentality still exists in the HIV service world, and it is in part the basis of my work today.
This is dangerous, not just because it risks major burnout early in our careers. It also means that in an effort to make a name for ourselves in this field—partly because our options often seem limited in other professions—we may use what few friendships we have in ways that advance our professional work and allow us to meet the demands of our funders. This may be great for a career, but it can be hard on friendships.
Boom
Tokenism, isolation and control represent the T-I-C in tic. The boom represents the increased personal risk BMSM service providers encounter while navigating the duality of our lives. We must exist as professional tokens while trying to engage in social and romantic relationships that will not compromise the expectations of our employers.
America’s HIV crisis didn’t just facilitate the coordination of HIV services. It also generated a cadre of well-intentioned, community-based institutions that fought to remain relevant despite deficiencies in key areas (e.g., organizational development, fundraising and human resource development).
Many of these organizations are funded to work with vulnerable communities with at-risk behaviors. The most common way to access these high-risk groups is to employ members from these same vulnerable communities.
So what responsibility does the HIV organization have as it relates to the overall wellness of BMSM service providers? The same responsibility it has when working with any vulnerable community.
Our Upcoming Webinar: Promoting Healing
My story is one of many. For the first time, these stories are coming together to promote healing, wellness and truth-telling for BMSM service providers and the organizations that employ them.
This November, ETR’s Community Impact Solutions Program (CISP), along with other capacity-building and technical assistance providers, is gearing up to support a CDC-initiated strategic planning effort. We’ll be reaching out to organizations recently funded to do comprehensive high-impact HIV prevention. These organizations are targeting HIV-negative individuals who engage in high-risk behaviors, or focusing on services for HIV-positive individuals.
On November 9, CISP will be offering our first of four BMSM-focused webinars for our Wellness Webinar Series, supporting organizational wellness and sustainability. (By the way, everyone is invited to participate in these webinars, not just funded organizations—see below.)
Intentional Leadership: Doing the Work and Being the Work is the introductory webinar. We will discuss the findings from a small inquiry of BMSM service providers who have shared their stories about navigating this field in dual roles as service providers and members of the target population.
Answering Our History
HIV is a social disease that affects us on many levels. The modern day HIV/AIDS workforce was founded in crisis, typically by groups most affected by the disease. Early on, there was little support coming from beyond those communities.
The emergency these groups experienced during the initial outbreak left many newly forged, community-based institutions with little time to be educated about how to run an organization effectively. In the early days, it didn’t take much for someone who was a skilled hairdresser, living paycheck to paycheck, to find himself or herself the head of a nonprofit with a large operating budget.
Capacity-builders recognize this historical foundation. They are actively seeking to fill the gaps that still show up within agencies today. Recently, the Black AIDS Institute released a report discussing some of the HIV literacy issues currently faced by this workforce.
The Call: A Higher Standard of Practice
We encourage executive directors and anyone who hires BMSM service providers, as well as individuals who fund these programs, to come and learn ways to best support this group. Find out how your agency can incorporate healthy tools and practices for BMSM service providers, BMSM clients and your agency as a whole.
Attending this webinar means that you are concerned for the well-being of BMSM. It means you are ready to learn about our perception of truths—and that might incite some uncomfortable feelings. It also means you are calling yourself and your agency to a higher standard of practice around trauma-informed employment strategies for BMSM and BMSM service providers.

As we move into potentially another 30-plus years of combating HIV/AIDS, we can identify and apply lessons learned, strengthen our workforce and prioritize the health of those who do this work. I hope you’ll join us in the webinar to help move this part of the work forward.
Learn more about the webinar here.
Michael Everett, MHS, is a Project Coordinator and HIV/Sexual Health Trainer working with ETR’s Community Impact Solutions Program. He is also CEO at Intimacy & Colour, LLC. He can be reached at michael.everett@etr.org or found on LinkedIn.



